

Background: Gene therapy for hemophilia A is designed to be a one-time infusion to deliver functional copies of the defective factor VIII (FVIII) gene, to facilitate the endogenous production of therapeutic FVIII levels. The aim is to achieve long-term protection from bleeds without the burden of regular infusions.
Aims: To better understand patients' experiences of living with hemophilia A, the impact of traditional hemophilia A treatments, and patients' perceptions of the potential value of gene therapy versus traditional prophylactic treatments.
Methods: Patients were identified from the database of a US rare diseases patient organization, who also recruited and screened patients for the study using materials developed by the outcomes research organization (RTI-HS) and Takeda. Adult males aged ≥18 years with a self-reported diagnosis of moderate or severe hemophilia A, who reported using factor or nonfactor prophylactic treatment and were not currently receiving treatment for inhibitors, were eligible for the study. Eligible patients provided verbal informed consent to participate in a semi-structured, 60-minute telephone interview conducted in English by 2 members of RTI-HS who did not have access to any patient-identifying information at any time during the study. Targeted questions probed perceptions of treatment burden, impact of hemophilia A on daily life, and time spent on treatment. Additionally, questions were posed to assess patients' perceptions of the impact of traditional treatments and the potential benefits they anticipate from gene therapy.
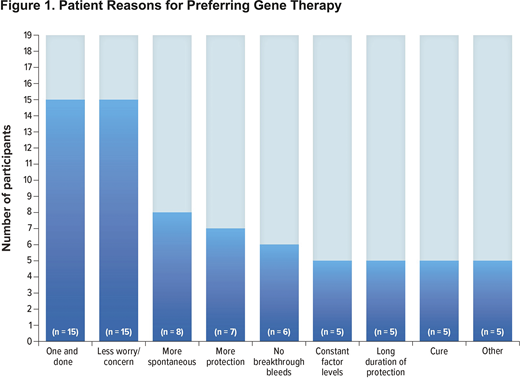
Results: Nineteen patients aged 19-55 years with moderate (n = 1) or severe (n = 18) hemophilia A were interviewed. Most (16/19, 89.5%) received prophylactic FVIII therapy, (3/19, 15.8%) were receiving nonfactor prophylactic treatment, of which 1 patient also used FVIII treatment. The aspects of current or past treatments most frequently disliked by patients were lack of efficacy, frequency of infusions, intravenous administration, vein health/scar tissue, and dosing volume. Most patients expressed satisfaction with their current treatment (18/19; 94.7%), though all listed ≥1 negative treatment impact, most frequently related to difficulties with travel (13/19; 68.4%), mood/emotions (12/19; 63.2%), day-to-day activities (10/19; 52.6%), and physical health/activities (7/19; 36.8%), including having to give up or reduce particular activities because of their treatment and needing to be more cautious, especially on nontreatment days. When presented with a hypothetical scenario for gene therapy - a one-time long-acting intravenous infusion to provide a constant level of FVIII that could reduce future bleeds - all patients stated they would choose gene therapy over their current therapy, although several said they would have initial questions regarding safety, efficacy, and duration of protection. Commonly expressed reasons for preferring gene therapy (Figure 1) included fewer infusions and less worry about the need to infuse. All 19 patients said they expected to be highly satisfied with this treatment, largely because of the long-term protection from bleeds, fewer infusions, and less concern about inhibitors. The most commonly anticipated improvements were in mood/emotions (15/19; 78.9%), specifically related to reduced concern about infusions and bleed protection. Other commonly anticipated improvements included gain in time usually spent infusing (13/19; 68.4%), easier travel (12/19; 63.2%), and improved physical health and ability to perform activities (10/19; 52.6%).
Conclusions: This study identified specific patient priorities, including treatment convenience, long-lasting bleed protection, frequency of intravenous infusions, and infusion volumes. The results suggest that gene therapy clinical trials should consider evaluating patient concerns in relation to the level of patient confidence in bleed protection. A study limitation is that, at the time of the survey, data on the efficacy and safety of gene therapy were limited. In the future, the study will be expanded to include a larger population of patients with hemophilia.
Sun:Takeda Pharmaceutical Company Ltd.: Current Employment. Olayinka-Amao:Takeda Pharmaceutical Company Ltd: Other: RTI-HS was contracted by Takeda Pharmaceutical Company Ltd to conduct this work; RTI Health Solutions: Current Employment. DiBenedetti:RTI Health Solutions: Current Employment; Takeda Pharmaceutical Company Ltd: Other: RTI-HS was contracted by Takeda Pharmaceutical Company Ltd to conduct this work.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal